Disclaimer:
The content on this website is for informational and educational purposes only and is intended to help readers understand AI technologies used in healthcare settings. It does not provide medical advice, diagnosis, treatment, or clinical guidance. Any medical decisions must be made by qualified healthcare professionals. AI models, tools, or workflows described here are assistive technologies, not substitutes for professional medical judgment. Deployment of any AI system in real clinical environments requires institutional approval, regulatory and legal review, data privacy compliance (e.g., HIPAA/GDPR), and oversight by licensed medical personnel. DR7.ai and its authors assume no responsibility for actions taken based on this content.
Clinicians are no longer asking “Should we try an ambient AI scribe?”, they’re asking “Which one can I safely deploy at scale without wrecking my workflows or my compliance posture?”
In this 2025 comparison, I walk through how ambient AI scribes work, then dig into Abridge, Suki, and Ambience Healthcare from the lens I use when advising health systems: real‑world accuracy, integration depth, security, and total cost of ownership, not just marketing demos.
All insights are based on current public information as of December 2025, vendor documentation, peer‑reviewed literature (e.g., NEJM Catalyst, JAMA Network Open), and my own implementation experience. This isn’t medical advice or a buying directive, it’s a technical guide to help you ask sharper questions and de‑risk your next pilot.
Table of Contents
Understanding Ambient AI Scribes (Ambient AI Scribe Comparison Essentials)
How Ambient Clinical Documentation Works
Ambient AI scribes sit in the background of a visit, usually via microphone in the exam room or a telehealth feed, and:
- Capture clinician–patient audio (often multi-channel, sometimes with device metadata).
- Transcribe using medical ASR (automatic speech recognition) tuned for accents, noise, and clinical vocabulary.
- Structure and summarize with LLMs and task-specific models into SOAP notes, HPI, ROS, assessment/plan, orders, and patient instructions.
- Write back into the EHR via FHIR APIs, HL7, or native integrations.
A typical pipeline I see in production:
- Low-latency ASR on-device or nearby GPU
- Streaming diarization (who said what)
- LLM-based abstraction constrained by templates, ontologies (e.g., SNOMED, ICD-10), and guardrails
- Human-in-the-loop review (clinician sign-off is mandatory: these are not autonomous notes)
Recent work in JAMA Network Open (2024) and NEJM Catalyst (2023) has shown that well‑implemented ambient systems can cut documentation time by 30–50% while maintaining chart quality, though results vary by specialty and deployment quality.
Why Clinicians and Health Systems Rely on AI Scribes
From what I’ve seen in rollouts across IM, FM, and cardiology:
- Burnout relief: Physicians routinely report reclaiming 1–2 hours per day previously spent on after-hours charting.
- More eye contact, less keyboard: Ambient AI scribes reduce the “laptop wall” between clinician and patient.
- More complete documentation: Systems often surface overlooked details (e.g., negative ROS, counseling time) that matter for quality metrics and risk adjustment.
- Financial upside: Better coding capture and fewer missed elements can improve revenue integrity.
But health-AI teams care about different questions:
- PHI handling under HIPAA/GDPR (data residency, BAA, encryption, retention windows)
- Hallucination and omission rates under real-world noise
- Latency (can the note be ready before the clinician leaves the room?)
- EHR integration depth and operational overhead (SAML, device fleet, support load)
The rest of this ambient AI scribe comparison centers on those operational details rather than generic feature lists.
Abridge Review — Clinical-Grade Ambient AI Scribe for 2025
Core Capabilities and 2025 KLAS Award Insights
Abridge has positioned itself squarely as a health-system–grade ambient AI scribe. In early 2025 it received the inaugural CHIME–KLAS Trailblazer Award for Healthcare AI Innovation, which mainly reflects strong health-system referenceability rather than raw model novelty.
Key capabilities, based on deployments and public reports:
- Deep Epic integration with co-innovation programs and native in-chart workflows
- Visit-level summaries structured as SOAP notes, problem-based plans, and patient-friendly after-visit summaries
- Specialty tuning (cardiology, primary care, oncology, and more) with templates and phraseology aligned to standard practice
- Configurable prompting and templates per service line, crucial when aligning to local note styles and regulatory documentation rules
In NEJM Catalyst (2023) and subsequent case studies, ambient systems like Abridge have been linked to reduced documentation burden and improved provider satisfaction, though the exact impact is site-specific.
From my own perspective, Abridge’s main strength is consistency in large, complex Epic environments. The teams I’ve worked with report relatively predictable behavior once workflows are stabilized.
Pricing Model, Compliance, and EHR Compatibility
Abridge typically prices as per-clinician-per-month enterprise contracts, sometimes tiered by:
- Number of encounters
- Depth of integration
- Additional modules (e.g., patient summaries, specialty packs)
Actual numbers are under NDA, but it’s safe to assume enterprise SaaS pricing, not solo-practice budget.
On compliance and trust:
- HIPAA-compliant with BAAs, encryption in transit and at rest, and configurable retention
- Public commitment to working within US and EU privacy frameworks: always confirm data residency if you’re under GDPR
- Designed for Epic-first, but also supports other EHRs (e.g., Cerner/Oracle, athenahealth) via standards-based integration where deeper native hooks aren’t yet available
If you’re an informatics lead inside a large US health system on Epic, Abridge belongs on your short list simply because the path of integration resistance is lower than with many competitors.
Suki Review — Voice-First AI Scribe for Flexible Clinical Workflows
Mobile-Optimized Dictation and Voice-First Design
Suki started closer to a smart dictation assistant and has evolved into an ambient scribe while preserving its voice-first DNA. For many clinicians, that’s a feature, not a bug.
In practice, I see Suki used in two main modes:
- Ambient capture of the visit, followed by AI-generated notes
- On-demand voice dictation on mobile or desktop, with commands like “Suki, create an HPI for…”
For specialties that move around a lot (hospitalists, orthopedics, urgent care), the mobile-first design is a real advantage. Suki’s recent enhancements in 2025 also extend to multi-language support and more robust noise handling, as covered in trade press reports.
Coding, Billing, and Revenue Cycle Support
Where Suki stands out in this ambient AI scribe comparison is tight coupling to coding and billing:
- AI-assisted ICD-10 and CPT suggestion based on visit narrative
- Detection of documentation gaps that affect level-of-service determination
- Support for HCC/risk capture, which is particularly valuable in value-based care contracts
A recent report in MobiHealthNews highlighted Suki’s expansion into clinical coding capabilities, aiming to reduce coder workload and improve revenue integrity. Of course, coders still need to review and validate, this is decision support, not automated billing.
For health systems with significant documentation-related denials, Suki can be positioned as both a workflow and revenue intervention, which can help justify the business case internally.
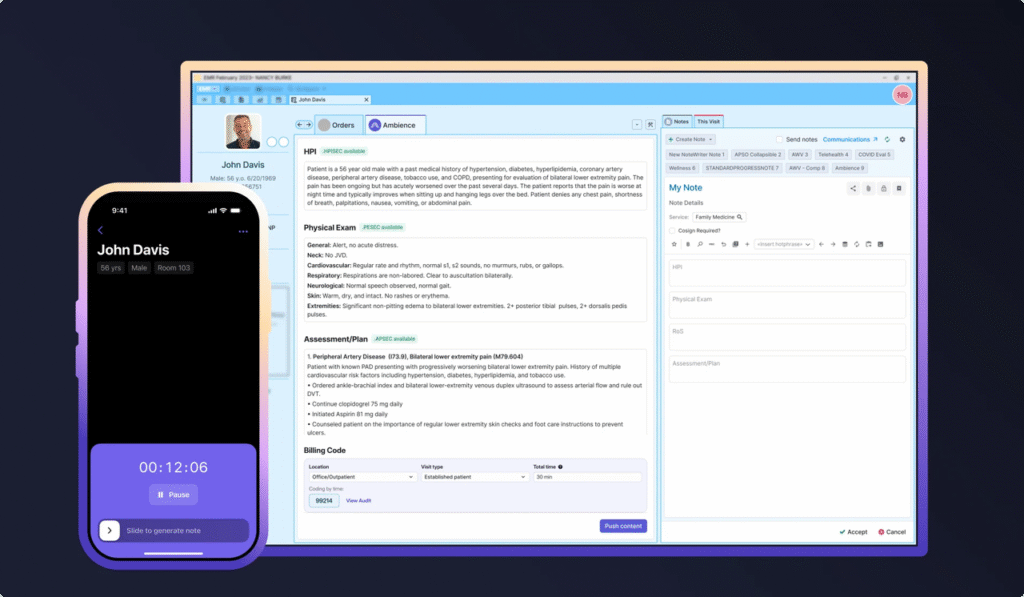
Ambience Healthcare Review — Enterprise-Ready Ambient AI Scribe
Epic-First Deployment and System-Level Integration
Ambience Healthcare has taken an enterprise-architecture-first approach. In 2025, Epic added Ambience to its AI “toolbox” program, and Ambience has been highlighted in mainstream press including CNBC and STAT as a leading ambient AI player.
What I see in real deployments:
- Designed to be deeply embedded into Epic workflows, including in-note editing, order suggestions, and task routing
- Strong emphasis on low latency, many clinicians report having a draft note ready before leaving the room
- Tooling that’s friendly to IT and security teams: centralized configuration, SSO/SAML, device posture checks, and detailed audit trails
For health systems that want to standardize not just notes, but system-level workflows across service lines, Ambience’s architecture is attractive.
Multi-Specialty Accuracy and Scalability
Any ambient AI scribe lives or dies on accuracy and resilience:
- Multi-specialty tuning: Ambience markets support for a wide range of specialties (ED, surgery, pediatrics, behavioral health). In my experience, performance is strongest in high-volume general specialties first, with sub-specialties improving over time as data and feedback accumulate.
- Scale characteristics: Ambience has been deployed across large networks, which matters if you’re planning a 1,000+ clinician rollout.
Some early observational data (e.g., in STAT’s 2025 coverage) describe reductions in after-hours charting and burnout when ambient scribes like Ambience are adopted, but we still need more head‑to‑head, peer‑reviewed trials to separate product effects from implementation quality.
Technically, Ambience is a good fit when your CIO asks, “Can this scale across our enterprise without spawning one-off shadow IT?”
Abridge vs Suki vs Ambience: 2025 Head-to-Head Comparison
Real-World Accuracy, Latency, and Documentation Speed
From combined literature and field experience, here’s how I’d characterize the three, recognizing that exact metrics will vary by site, mic setup, and specialty:
- Abridge: Strong on structured, guideline-aligned notes, especially in Epic. Accuracy is high when audio quality is good: hallucinations are usually stylistic rather than clinical, but you must still monitor for omitted negatives and misattributed statements.
- Suki: Excellent speech recognition and command handling, especially for mobile dictation. Ambient performance is solid, but I see slightly more physician editing in complex, multi-problem visits. Latency is acceptable but can trail enterprise-optimized setups when network conditions are poor.
- Ambience: Optimized for speed and inline editing. Many clinicians report minimal lag: but, like all LLM-powered tools, it can still produce speculative statements if the audio is ambiguous. Guardrails and domain constraints are critical.
In a recent JAMA Network Open 2024 trial of an ambient scribe (not vendor-specific), note completion time decreased significantly but error types shifted from missing data to misclassification. I advise teams to build ongoing QA dashboards: track error class, hallucination rate, and clinician-edit deltas by specialty.
Transparent Pricing Comparison Table
Vendors change pricing frequently and most enterprise numbers are under NDA, but based on public info and typical deals, the landscape in 2025 looks roughly like this (for US markets):
| Vendor | Typical Fit | Pricing Style* |
| Abridge | Large IDNs, Epic-heavy environments | Per-clinician/month, enterprise tiers |
| Suki | Small–mid groups, mobile-heavy use | Per-clinician/month, some smaller tiers |
| Ambience | Large systems, multi-specialty scaling | Per-clinician/month, enterprise-only |
*Indicative only. Not official quotes. Always confirm with vendors and legal.
For solo or micro practices, list prices can be prohibitive unless the vendor offers a specific SMB product. For large systems, the real question isn’t sticker price, it’s total cost of integration, change management, and governance.
EHR Integration Depth: Epic, Cerner, Athena, and More
A quick integration-oriented view:
- Epic: All three vendors integrate with Epic: Abridge and Ambience have particularly deep collaborations and native workflows.
- Cerner/Oracle Health: Generally supported via FHIR/HL7. Depth varies: expect more custom work and close vendor collaboration.
- athenahealth, eClinicalWorks, others: Suki and Abridge are more visible here: Ambience is catching up but is still perceived as Epic-first.
When I evaluate ambient AI scribes, I don’t just ask “Is there an integration?”, I ask:
- Is the note created as a first-class clinical document or pasted text?
- Can the system pre-populate problem lists, orders, and diagnoses (with human sign-off)?
- How do edits in the EHR flow back to model learning or configuration?
Those answers matter more than whether there’s a logo on the vendor’s integration page.
How to Choose the Right Ambient AI Scribe (2025 Guide)
Best Options for Solo Practitioners and Small Clinics
If you’re running a small clinic, your constraints are usually cash, IT bandwidth, and flexibility.
In that setting, I’d look for:
- Simple web/mobile capture with minimal device management
- Clear, published pricing with short-term contracts
- Lightweight EHR connectivity (even if it’s semi-manual at first)
Suki often fits best here because of its voice-first mobile design and more accessible footprint. Abridge can work for groups that are part of a larger network where the system is negotiating enterprise pricing and rolling out shared infrastructure.
Before going live, I recommend a 4–6 week pilot with:
- Baseline and post-pilot measures of documentation time and after-hours charting
- Independent QA review of a random sample of notes for clinical accuracy and hallucinations
Best Options for Hospitals, Networks, and Large Health Systems
For large systems, the choice is less about UI preference and more about governance, security, and scale.
Patterns I’ve seen work:
- Epic-heavy IDNs often shortlist Abridge and Ambience first due to integration depth and enterprise tooling.
- Systems with a lot of mobile, cross-site workflows sometimes bring Suki in for specific service lines while another vendor handles core inpatient/ambulatory.
My selection checklist usually includes:
- Security & compliance: Detailed review of hosting, encryption, access controls, PHI flows, and audit logging. Confirm HIPAA BAAs and GDPR alignment where applicable.
- Model behavior: Specialty-specific evaluation sets, red-teaming for hallucinations, and clear escalation paths for safety issues.
- Operational readiness: Training plans, super-user networks, and incident management.
Medical & Regulatory Disclaimer (Read This Part)
I’m sharing this ambient AI scribe comparison for informational and educational purposes only. It doesn’t constitute medical, legal, or billing advice, and it’s not a recommendation to use, or not use, any specific product. Ambient AI scribes can make errors, including omissions, hallucinations, and misclassification of clinical details.
- Clinicians must always review, edit, and sign notes: never let AI-generated documentation stand without verification.
- Do not use these tools for emergency triage or life‑threatening situations. In any medical emergency, follow your local emergency protocols immediately.
- Always consult your organization’s compliance, legal, and information security teams before deploying AI that touches PHI.
I have no financial relationships, equity, or consulting contracts with Abridge, Suki, or Ambience Healthcare as of December 2025.
Frequently Asked Questions
What is an ambient AI scribe and how does it work in clinical settings?
An ambient AI scribe passively listens to clinician–patient encounters via room or telehealth audio, converts speech to text with medical ASR, then uses LLMs to structure SOAP notes, HPI, ROS, and plans. The draft note is written back to the EHR through FHIR, HL7, or native integrations for clinician review and sign‑off.
How should I use this 2025 ambient AI scribe comparison to choose between Abridge, Suki, and Ambience?
Use the ambient AI scribe comparison as a checklist, not a verdict. Focus on real‑world accuracy by specialty, depth of Epic or other EHR integration, latency during live use, security posture (HIPAA/GDPR, BAAs, audit logs), and total cost of ownership, including training, IT overhead, and change‑management effort.
Which ambient AI scribe is best for small practices versus large health systems?
For solo or small clinics, tools with mobile-first workflows and transparent pricing—often Suki—tend to fit better, especially when IT support is limited. Large Epic-heavy health systems typically prioritize Abridge or Ambience Healthcare because of enterprise-grade integrations, centralized administration, and better support for 1,000+ clinician deployments.
Are ambient AI scribes HIPAA compliant and safe to use with PHI?
Leading ambient AI scribes such as Abridge, Suki, and Ambience sign BAAs and provide encryption, access controls, and configurable data retention to support HIPAA compliance. Safety still depends on your implementation: validate notes regularly, monitor hallucinations and omissions, and ensure clinicians always review and approve AI-generated documentation before it enters the chart.
What are the main risks and limitations of ambient AI scribes in 2025?
Key risks include hallucinated or misclassified clinical details, missed negatives in ROS, latency in low-bandwidth environments, and workflow disruption if EHR integration is shallow. There are also regulatory and privacy concerns under HIPAA/GDPR. Mitigation requires pilots with QA review, specialty-specific evaluation sets, governance committees, and clear incident escalation paths.
Ready to test these models in practice? Get free API access to MedGemma and more on dr7.ai (limited-time Pro discount available).
Past Review:





